I recently put up a survey in a Facebook group full of Australian Psychologists. The survey asked:

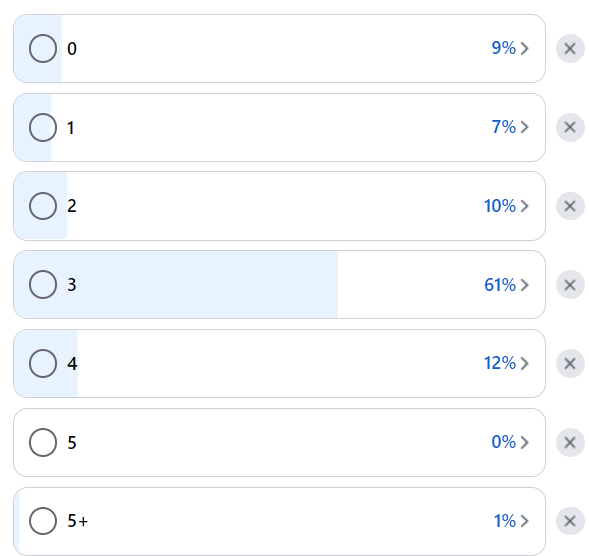
The options ranged from 0 to 5+ types of therapy. There were 112 respondents in total. By far, the number of interventions that the therapist respondents said we need was 3 – with 69 votes at 61%. Second place, which was 4 types of therapy, wasn’t even close at 12%. Third place was 2 types of therapy at 10% of the vote.
I found this so interesting. Why three kinds of therapy? Is that backed by research? Is it because three kinds of therapy feel safe; like a well-rounded sweet-spot?
Now this is hardly a scientific study, but a great way to get one thinking.
One day I might look into research on this, but not today. I tend to prefer asking questions and writing instead of researching. If anyone reading this has any potential answers, please let me know.
It wasn’t just the responses that provided important information, it was also the comments on the post as well. These comments gave me a good feeling, one of hope. As writing so much about trying to improve my outcomes as a therapist can make me fairly cynical. It was awesome to see people talk about the importance of the common factors and the therapeutic relationship in therapy outcomes. While I do often put our field in the crosshairs (and I’m about to do more of that today), it reminds me that there are so many therapists that believe in the importance of the therapeutic relationship.
Here is where I have been aiming my crosshairs. It’s not at individual therapists, but at our continued professional development system or continued education (CE system). Our CE system places far too much focus on alluring us into learning more interventions and kinds of therapy. We are not encouraged to deeply analyse the therapeutic relationship and know it extremely well – to master it. It still boggles my mind that I struggle to find courses that solely target the therapeutic relationship, but I’ll find hundreds on learning the many kinds of therapy out there. In my view, our CE system is all backwards and it’s stopping us from effectively getting better outcomes.
If I was to give our CE system a motto it would be: “the more therapies you know, the more you will help your clients”. It will happily imply that you will never know enough, there is always more to know. If you don’t keep learning therapies you will be left behind. That’s one way of getting imposter syndrome to go out of its mind.
You can see for yourself, go onto the CE course directories like those for the APS and AAPI and you’ll see a lot on learning a kind of therapy, you’ll be so spoiled for choice, but there will be hardly anything, if anything at all for the therapeutic relationship. It’s my belief that when you’re doing a course in a kind of therapy, 90% of the content is in interventions, skills and tools and 10% on therapeutic relationship factors at best. It’s a major reason why I haven’t undertaken a course in any kind of therapy for almost three years now. I remember the last course I took in ACT therapy, it did talk about client goal alignment. Funnily enough, it taught something I now completely disagree with. The course said I shouldn’t let a client choose a ‘dead person’ goal (which is a goal only a dead person could achieve), e.g. “I want to stop my anxiety”.
I feel the opposite way, I allow dead person goals. When a client expresses a goal like that, there’s no pushback from me whatsoever (assuming the client and others are safe). Not even comments from me about how we should be aiming for “manageable anxiety” or “everyone has anxiety, at least to some degree”.
My point is, that the most important lesson I have ever learnt about improving my engagement with the therapeutic relationship would never come from a course for a kind of therapy. There’s no way that a course would tell me that allowing dead person goals from a client are ok.
Scoff, if you must, but allowing dead person goals, has been a major factor in me improving my outcomes. I believe that wholeheartedly… and the only way I learnt it was from practice based evidence. From listening to my clients.
Allowing dead person goals is a great strategy for responding to clients who are very concrete in their goals. You don’t want to challenge those clients too early, before you have their trust, that’s a recipe for drop out.
On the rare occasion, when I get a client saying things to me like that I am the best therapist they have seen, by far. It’s not because of my interventions. It’s because I have focused my attention and systems on really listening to them as much as possible and doing my best to go with what they want, not what I think they want or need.
There will be a few of you reading this thinking something like: “well I do what you’re talking about. I ask clients what their goals are. I ask my clients if what I am thinking is accurate. I check in with them”. To be clear, I’m not saying anyone is bad at client alignment, most of us are great, but my point is that we could be far better. If I have been able to work on it for three and a half years after registration, I can almost guarantee you will have room to grow here as well. Unfortunately no, it won’t be gained with more experience either – you’ve got to really work at it.
In fact, if I include three more variables, ones that I feel have been important for me as a therapist:
- Deep listening (DL) – including giving a client what they want.
- Therapy orientation (TO) – the amount we know about providing a kind(s) of therapy.
- Self acceptance (SA) – How much we accept ourselves, not just as a therapist, but as a person.
- Collaborative problem solving (CPS) – the likelihood that interventions built with a client will contribute to symptom reduction/increasing well-being for a client.
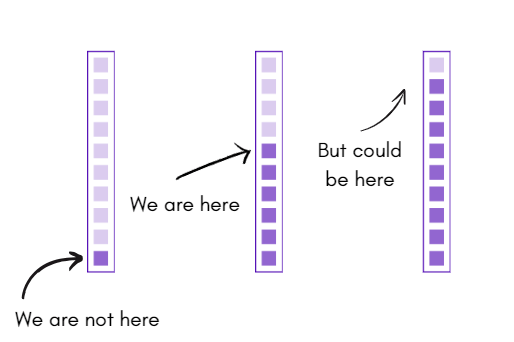
This is where I feel like we sit as a field, on those four variables, it’s not based research, but a lot of gut feeling and observations:
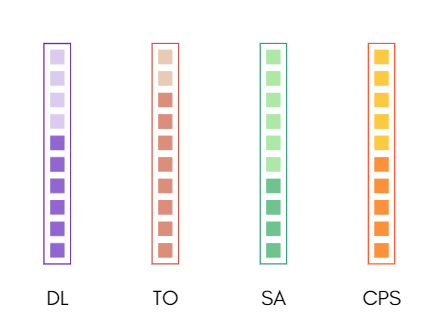
We are great listeners, better than most people at least, we know a lot about at least one kind of therapy, our self-acceptance is on the lower side (at least early career) and our interventions may work at least half the time on average.
I believe though that in order to improve, the answer isn’t in knowing more therapies once you are already competent there. It’s in just being able to listen really, really, really well to clients – what I have started referring to as deep listening (which includes giving the client what they want).
I know that none of us are master listeners, because it’s a skill like anything else and skills need lots of practice to improve. We don’t give enough attention to actually practising listening, in order to keep developing it.
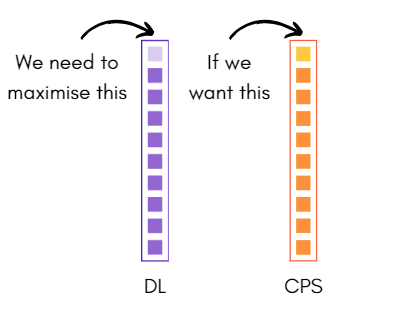
We all want to help our clients to get better faster. We all care a lot, but I clearly think we are putting our eggs into the wrong baskets. If we want to CPS to be a home run more often, the only way we get there, in my view, is like this:
Does all this mean I see interventions as completely unimportant? Not at all – quite the opposite in fact. Most client’s want tools and strategies at the end of the day.
At it’s worst, the CE system can churn out some really bad therapists. The worst kind of therapist, in my view, is one that thinks they listen well but all their focus is on therapy orientation. I have lived experience as a client in that very situation. I had a therapist who kept asking me what I wanted, but when I answered would then ignore my request, to instead give me more psychoeducation. I felt like I had no voice. I stopped going after almost crying after the second session because I felt so unheard – which was the exact reason I went to therapy in the first place. I never ever, ever want to be that therapist.
I now assume rightly or wrongly that when a client isn’t clicking with homework or improving as much as hoped, its because I haven’t listened as well as I thought I was. So I reset. Put my tools down… and listen. It’s that simple. I lean on seeking clarification, which I dial up to eleven.
This is where I think I sit after three and a half years of Deliberate Practice. Focusing on goal alignment with clients, finding ways to listen more consistently and deeply, while also finding ways to accept myself more (most of the time accidentally):
I have the outcome statistics to back me up as well, it has taken a while, but I’m now averaging 10 sessions (up from 4 sessions in 2021 with my closed cases and 24 sessions with active clients (up from 6 sessions in 2021) and my relative effect size has crossed above 0 for the first time ever.
So to wrap up with a final message, yes you need to bring something to the table, clients pay us to do more than listen and build a good relationship alone, but once you have enough therapy knowledge, don’t keep adding more because our CE system tells you to. Stop – step back – turn to your client and ask: “you know what, what would you like?”. If they want dessert for dinner then so be it. Don’t bring anything in until you know truly and deeply what your client truly wants.

5 responses to “Yes we attend to the therapeutic relationship well, but it could be even better”
My BF and I were talking about this earlier today. He was focused on the individual tratment of therapy. I shared that the individual is universal which is often true which allows us to use modalities to address issues. However, there are also individual issues with each client that need to be attended to. Some of these issues are specific triggers, attachment/connection specifics and memories, building ego strengths and identifiying values has to be individual to the client as well. All of these are very complex but important in the therapeutic relationship.
I do believe that as we move forward in more sophisticated ways we are learning that CEU’s about modalities is not where it is at for improving treatment. It is about knowing our weaknesses, honing skills through deliberate practice, being able to hold intensity and our own countertransference (which mamy current therapists that I know are completely unaware of), keeping knowledge about he individual client in our minds as wel use both universal and individual conceptualizations of treatment.
Additionally, with Value Based Health Care on our horizon, there will be more consumer focused paramaters and benchmarks for us to monitor which will be the result of our own abilities. Man is this scary, right…
There is such depth and breadth to be tapped into about these issues for CEU’s and I cannot wait to see what comes up.
LikeLike
Get me off your list. Unsub doesn’t work!!!!Harry Korman
LikeLike
Hi Harry
Really sorry about that – I had no idea the unsubscribe doesn’t work!
I removed your email address.
Jimmy
LikeLike
Fantastic read,
It’s amazing to me the heavy emphasis on the scientific and evidence based components of psychology, only to find that much of practice hardly involves any.
From my perspective you are paving the way for us to think more deeply and empirically about therapy – something that is quite rare it seems at least from the algorithms that have been feeding my info.
Very keen to see how AI can be implemented into this process as it evolves and become more and more capable.
As an aspiring psych I have learnt much and have great respect for you Jimeoin!
Best,
Riley Thomson
LikeLike
Thanks Riley – I’m chuffed to hear that. That’s exactly it, I just want to try and encourage people to try look at things differently. To lean more on sources of information of therapy that we don’t get taught to. What better source of info than the person receiving the service?
LikeLike